1. Summary
Note that fractures of the thumb metacarpal require special consideration: see thumb fracture guideline
2. How are they classified?
These are classified as closed or open, by which digit is injured, by anatomical site of fracture (base, shaft or neck), and by displacement/angulation
3. How common are they and how do they occur?
Metacarpal fractures are a common injury in older children and adolescents, particularly the little and ring fingers. They usually occur due to a blunt force applied to a clenched fist such as punching a fixed object or from falling onto a closed fist.
4. What do they look like – clinically?
There is usually significant bruising and tenderness in the part of the hand corresponding to the fracture site.
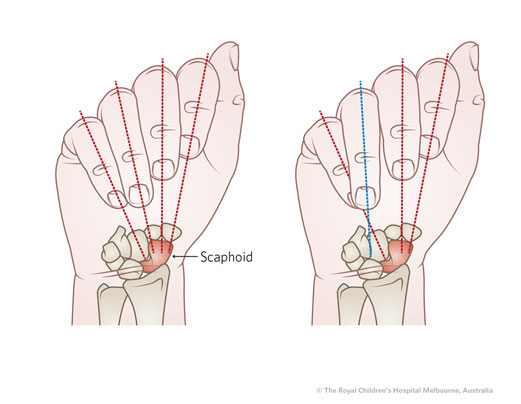
There may be rotational deformity, which is best identified by having the patient flex her fingers into a loose grip. Looking for ‘scissoring’ or overlap of the fingertips. This is demonstrated in the image below., with the normal exam at left, and rotational deformity of the ring finger shown at right.
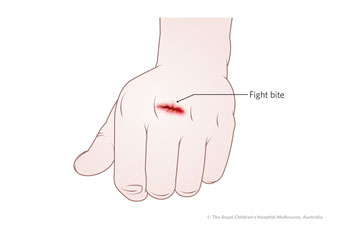
An open wound over the dorsal aspect of the metacarpal head may suggest a “fight bite”. This occurs when a tooth penetrates the MCP joint; Risk of deep infection here is very high, regardless of whether abnormality is present on the xray: surgical admission for exploration and washout is indicated.
5. What radiological investigations should be ordered?
AP, lateral and oblique films of the hand
6. What do they look like – on X-Ray?
|
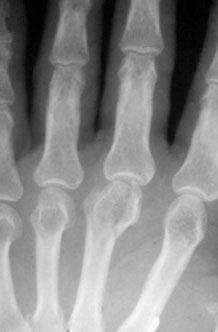
Metacarpal neck fracture
(sometimes labelled a “Boxer’s Fracture” when found in little finger metacarpal) |


Left: neck fracture little finger metacarpal
Right: neck fracture middle metacarpal |
|
Metacarpal shaft fracture |
 |
|
Metacarpal Head Fracture |
 |
|
Metacarpal Base Fracture
To better appreciate any dorsal subluxation in these injuries, a lateral or oblique view should be examined |
 |
For Fractures of the Thumb metacarpal see thumb fracture CPG
7. When is reduction (non-operative and operative) required?
As a loose guide for shaft fractures (there are many other factors at play here):
- For Index and Middle metacarpals: >10 degrees of angulation, or any rotational deformity
- For Ring metacarpal: >15 degrees of angulation, or any rotational deformity
- For Little Metacarpal: >20 degrees of angulation, or any significant rotational deformity
For metacarpal neck fractures (i.e. the 5th metacarpal neck “Boxer’s Fracture”), greater degrees of apex-dorsal angulation may be accepted, so long as the clinical examination doesn’t reveal findings of malrotation, extensor lag (‘pseudoclawing’), or ‘MC head in the palm’ (palpable MC head because of angulation, felt palmarly) .
Fractures at the head or base of the metacarpal should not be manipulated in the ED.
8. Do I need to refer to Hand Surgery now?
- Open fractures (including fight bites as illustrated above - any laceration over the metacarpal heads should be treated as highly suspicious for these injuries. Urgent exploration and washout is required)
- Neurovascular compromise
- Multiple fractures in a crushed hand.
- Delayed presentation of injury.
Other injuries can be followed up in Hand Surgery clinic within the next 7 days.
9.What is the usual ED management of this fracture?
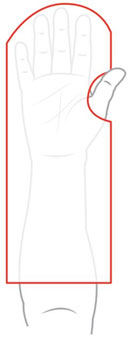
Closed metacarpal injuries not needing reduction should be splinted in the safe hand position (Wrist in 20 degrees of extension, MCP joints in 70 degrees of flexion, IP joints in full extension)
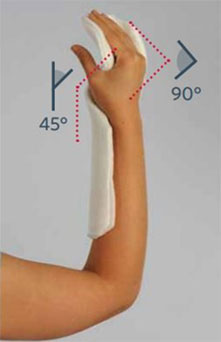


Where required, reduction can take place under procedural sedation and/or regional anaesthesia. After applying some longitudinal traction to the digit, the MCP is flexed to 90 degrees and then axial loading applied to the proximal phalanx to correct any flexion angulation. The hand is then splinted in the safe hand position as above.
10. What follow-up is required?
Follow up should be arranged in hand surgery clinic in approximately one week – at RCH, this is the Plastics Dressings clinic . Discuss with the on-call registrar to ensure this appointment is appropriately timed.
If the referral is delayed, please contact the hand surgery clinic.
11. What advice should I give to parents?
Elevation of the limb, typically in a sling.
Avoid activities involving the possibility of heavy impacts on the hand or cast, such as sports.
Plaster care advice.
12. What are the potential complications involved with this injury?
Unrecognised/uncorrected rotational deformity can result in significant functional hand impairment
“Fight bites” that are not recognised or addressed early can result in septic arthritis or infections of the deep spaces of the hand.
Arthritis may complicate any intra-articular fracture of the metacarpal base or head.
13. References
Cornwall, “Paediatric Finger Fractures: Which Ones Turn Ugly” J. Pediatr Orthop 2012;32:S25-31
Smit, A. “Fractures in the Child’s Hand” Current Orthopaedics 2006; 20:461-66
Nellans, K. et al “Pediatric Hand Fractures” Hand Clin 2013; 29(4): 569-78
Information Specific to Royal Children’s Hospital: Any metacarpal fractures requiring specialist input are handled by the Plastic Surgery team. RCH, the Plastic Surgery team. At some centres this may be an orthopaedic team; this guideline will refer to ‘hand surgery’ to encompass both specialty fields.
Last updated December 2020