See also
Resuscitation
Cervical spine assessment
Key points
- Most cases of drowning result in minimal or no respiratory impairment and do not require hospital admission beyond a period of observation
- Cervical spine injury is uncommon but should be considered if there is a history of trauma eg diving
- The cause of drowning should be fully considered including medical causes or issues around supervision and safety
- Key principles of management are maintaining adequate oxygenation, preventing aspiration and stabilising body temperature
Background
Drowning is the process of experiencing respiratory impairment from submersion/immersion in a liquid
Terms such as "near-drowning," "secondary drowning," and "wet drowning" are no longer used and do not influence management
Assessment
History
Timeline
- Immersion time
- Time to and type of basic life support delivered
- Time to first respiratory effort
- Details of treatment used
Circumstances leading to the drowning. Consider the following:
- inconsistencies in story
- story incompatible with developmental age
Consider a medical cause for drowning in children who are competent swimmers, for example:
- seizures
- hypoglycaemia
- arrhythmias and Long QT Syndrome
- intoxication
Examination
- Evidence of hypoxic brain injury
- Evidence of respiratory compromise
- Signs of trauma particularly head and cervical spine trauma
Management
Investigations
Children who are asymptomatic and alert require no investigations
Further investigations should be guided by the history and clinical condition
- Chest X-ray findings do not correlate with clinical outcomes
- Altered mental state in the absence of significant hypoxia should prompt a search for reasons other than drowning as a cause, eg hypothermia, traumatic brain injury, co-existing medical condition, hypoglycaemia
- ECG may be helpful in diagnosing arrhythmias and Long QT syndrome
Treatment
Key principles of management are maintaining adequate oxygenation, preventing aspiration and stabilising body temperature.
Vomiting is common in drowning victims and aspiration of gastric contents is a major complication. Spontaneously breathing children should initially be placed in the lateral decubitus (recovery) position.
Prophylactic antibiotics have no role. Antibiotics have not been shown to improve outcome and should be restricted to patients demonstrating signs of infection or sepsis, or in the rare situation of submersion in grossly contaminated water. Please refer to
local antimicrobial guidelines
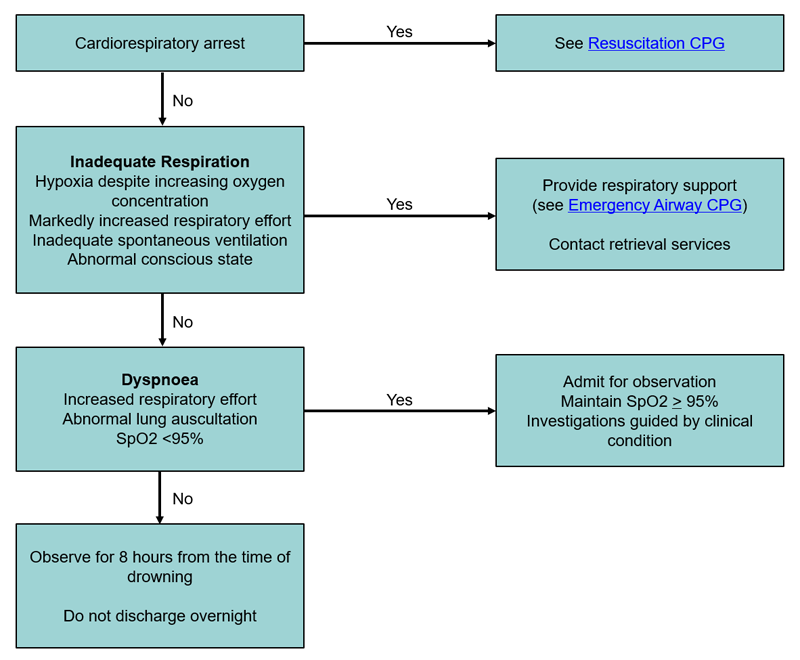
Treatment Flowchart
Hypothermia
- Hypothermia is a common complication of drowning
- Remove wet clothes and dry child
- Exposure should be minimised
- Active warming to normothermia should occur if core temperature is less than 34oC and there is no evidence of brain injury. This includes:
- warmed IV Fluids
- humidified oxygen delivery
- forced air warming blankets
There is some evidence for therapeutic hypothermia in children with hypoxic brain injury. This should be discussed with a Paediatric Intensivist
Consider consultation with local paediatric team when
- Increased respiratory effort
- SpO2
<95%
- Abnormal lung examination
- Underlying medical cause for drowning is suspected
Consider transfer when
- Persisting altered conscious state
- Respiratory compromise requiring assisted ventilation
- Ongoing hypoxia
For emergency advice and paediatric or neonatal ICU transfers, see
Retrieval Services.
Consider discharge when
- Observed for 8 hours from the time of drowning
- Asymptomatic
- Normal respiratory examination
- SpO2 ≥95%
- Education about water safety provided (see handout below)
- No ongoing safety concerns
- Referral to social work has been made if deemed appropriate
Parent information
Water Safety
Additional notes
Adverse prognostic indicators
- Submersion time >5 minutes
- Time to effective basic life support >10 minutes
- Arrival in hospital with CPR in progress
- GCS <5
- Rectal temperature <30oC
- Arterial blood pH <7.1 on arrival
Last Updated June 2020