1.
Summary
Metatarsal fractures are common in the paediatric population and rarely require operative management.
Care should be taken in differentiating an avulsion fracture of the fifth metatarsal from a Jones fracture, due to the risk of nonunion in the latter.
2. How are they classified?
Metatarsal fracture are classified by the following:
- Open or closed
- Which digit is involved
- Location of fracture (base, middle, proximal metatarsal)
- Displacement and angulation
- Growth plate involvement (Salter Harris Classification)
3. How common are they and how do they occur?
Fractures of the metatarsals are common injuries in children.
Children 5 year or younger are more likely to fracture 1st metatarsal, whereas children older than 5yrs are more likely to injure 5th metatarsal
Common mechanisms of injury include:
- Fall from a height
- Sport related injury
- Inversion injury of ankle
- Crush injury caused by a heavy object falling onto the foot or motor vehicle tyre running over foot
- Axial loading
- Stress from heavy / repetitive intensive training
Fractures of the 2nd, 3rd and 4th metatarsals rarely occur in isolation and commonly result in fracture/s of the adjacent metatarsals. Occasionally, this is part of a LisFranc injury (tarso-metatarsal fracture-dislocation)
4. What do they look like - clinically?
The forefoot will usually appear swollen with bruising, and the patient may be unwilling or unable to bear weight.
5. What radiological investigations should be ordered?
Children with pain, swelling and/or deformity to forefoot require foot radiographs.
Plain film – anterior-posterior, oblique and lateral views
CT is seldom necessary. The exception is a suspected Lisfranc injuries, where it should be arranged in consultation with orthopaedics.
6. What do they look like on x-ray?
Fractures of the fifth metatarsal:
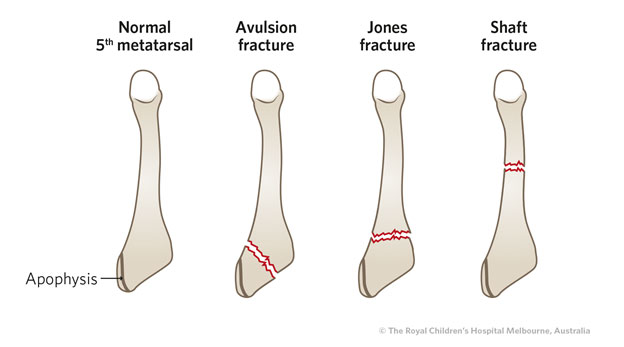
Figure 1 & 2: Normal 5th metatarsal films in 2 different 12 year olds. The apophysis (vertical lucency) is clearly visible on the right image - these are commonly mistaken for a fracture.
Figure 3 & 4: Two examples of 5th metatarsal avulsion fractures
Figure 5 & 6: AP and lateral image of a 'Jones Fracture' - an extra-articular fracture of the base of the 5th metatarsal. In contrast to the avulsion fractures, non-union in Jones fractures is common, so careful follow up is of high importance as discussed below.
Fractures of other metatarsals
 Figure 7: Undisplaced Fracture of 4th distal metatarsal head
Figure 7: Undisplaced Fracture of 4th distal metatarsal head
 Figure 8: Undisplaced fracture of 3rd and 4th metatarsals
Figure 8: Undisplaced fracture of 3rd and 4th metatarsals
 Figure 9: Minimally displaced first metatarsal fracture
Lisfranc injuries
Figure 9: Minimally displaced first metatarsal fracture
Lisfranc injuries
These complex injuries aretarso-metatarsal fracture dislocations which are caused by high force. The foot is usually very swollen and bruised and the patient is unable to bear weight, but x-ray features may be subtle. Widened tarsal-metatarsal joint spaces or space between the first and second metatarsal hint at significant injury. CT scan is required to clearly define the fracture/dislocation.
Figure 10 & 11: Xrays of two separate patient with LisFranc Fracture-dislocation, showing widened space between the first and second metatarsal, fracture at the base of the second metatarsal and avulsed fragment from the tarsal bones. The second patient also has a fracture of the cuneiform with a loose fragment, fractures of the 3rd and fourth metatarsals, and gross deformity.
7. When is reduction (non-operative and operative) required?
Operative management is required for:
- Significantly angulated or displaced fractures
- Multiple metatarsal fractures that are unstable
- Jones fractures. These are associated with a high incidence of non-union and re-fracture post cast removal due to the tenuous blood supply of this area. They may subsequently require fixation.
8. Do I need to refer to orthopaedics now?
Consultation on the day of presentation is required for:
- Open fractures
- Displaced fractures (>20 degrees of angulation or significant displacement)
- Multiple metatarsal fractures
- Suspected Lisfranc injury
- Jones fractures
- Neurovascular compromise
9. What is the usual ED management and follow up for these injuries?
Fracture type
|
ED management
|
Follow-up
|
|
Avulsion fracture at the base of the 5th metatarsal tubercle
|
Firm soled shoe or walking boot (CAM) if more support is required. Wear until able to walk without symptoms. This is usually 2-3 weeks.
|
No follow up required.
(If there in ongoing pain at the site at 2 weeks, see GP).
|
|
Jones Fracture of the proximal diaphyseal region
|
Refer to orthopaedics
Prone to non-union due to tenuous vascular supply
Children >13yrs prone to re fracture
|
Follow up in fracture clinic in 7-14 days
Early operative fixation will be considered at this appointment.
|
|
Metatarsal diaphysis- Undisplaced
|
Firm soled shoe or walking cast (CAM)
For 4-6weeks
Refer to orthopaedics if 20degress or more of angulation
|
No follow up required if undisplaced single metatarsal
|
|
Metatarsal diaphysis- Displaced
|
Minimally displaced- Below knee backslab
If completely displaced and / or 20degress or more of angulation, refer to orthopaedics
|
Follow up in fracture clinic within 7 days
|
|
Fractures involving the physeal plate (Salter Harris I-IV)
|
Below knee backslab
(consult orthopaedics if displaced)
|
Follow up in fracture clinic within 7 days
|
|
Lisfranc Injuries
May appear on X-ray as subtle fracture of first proximal metatarsal as described earlier
|
Refer Orthopaedics
|
CT foot; specialised orthopaedic management and follow-up.
|
9. What are the potential complications associated with these injuries?
- Non-union, and growth arrest are rare complications of metatarsal fractures in children
- If treated conservatively, Re-fracture of Jones fracture is possible post cast removal
- Unrecognised Lisfranc injuries may lead to chronic foot pain.
10. What advice should I give to parents?
- It is important to rest the foot, to keep it elevated for the first few days after injury and to apply ice for 20 minutes at a time several times a day.
- Regular simple analgesia for the first few days (for example, paracetamol and/or ibuprofen) is often indicated
- Undisplaced metatarsal fractures (except Jones fracture) heal very well: they are effectively internally splinted by the other structures in the foot, and often do not require specialist follow up
- Where are Jones fracture of the proximal fifth metatarsal has occurred, this requires close follow-up and consideration of internal fixation due to the significant chance of poor healing at the site.
11. References
Boutis, K., 2018. Metatarsal and toe fractures in children, UpTodate
Fox, S.M., 2018. Metatarsal fractures in children, PEM
Mahan, S., Hoellwarth, J., Spencer, S., Kramer, D., Hedequist, D., and Kasser, J. 2015 Journal of pediatric orthopaedics, 35, 3 296-302
Singer, G., Cichocki, M., Schalamon, J., Eberl, R., and Hollwarth, M. 2008 A study of metatarsal fractures in children. The journal of bone and joint surgery 90:772-6