1.
Summary
Fractures of the calcaneus often result from a fall from a height, and may be overlooked during the diagnosis and management of more obvious injuries including vertebral, pelvic, tibial and foot injuries.
As initial radiographs are frequently negative or have only very subtle abnormality, a high degree of suspicion is often required to make the diagnosis.
In most cases, with appropriate management paediatric calcaneus fractures have a favourable prognosis.
2. How are they classified?
- - Displaced vs undisplaced fractures
- -Intra-articular vs extra-articular
Displaced intra-articular fractures can further be described as tongue-type or depression-type.
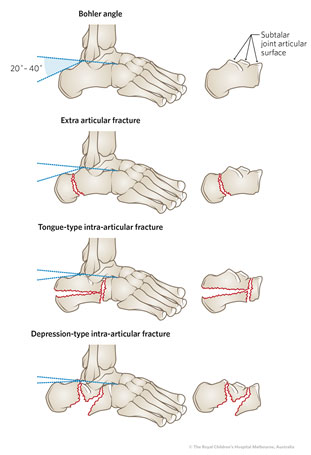
Calculation of Bohler's Angle is useful to evaluate collapse of the posterior facet of the calcaneus.
A line is drawn from the highest points of the anterior to the posterior facets, with another drawn from the highest point of the posterior facet to the highest point on the calcaneal tuberosity, as illustrated above.
The usual angle formed is 20-40 degrees. any angle significantly less than this suggests collapse of the posterior facet of the calcaneus. |
3. How common are they and how do they occur
- Calcaneus fractures are rare in children
- They usually occur from a fall from a significant height with axial loading of heel, injuries to the foot involving motorized vehicles or from direct blows to calcaneus.
4. What do they look like – clinically?
- Pain in the heel, with diffuse tenderness on palpation of the heel
- Swelling
- Plantar ecchymosis
- Skin abnormalities: open wounds, skin tenting, blistering
- Shortened and widened heel
5. What radiological investigations should be ordered?
In children, calcaneus fractures may be subtle and are often missed.
3 plain-film views of the foot: AP, lateral and oblique
Consider additional view: Axial (Harris) view, to assess talocalcaneal joint and plantar aspect of calcaneus
A CT scan may subsequently be required to assess for intra-articular involvement and fracture pattern, or where a high degree of suspicion remains following negative radiographs
6. What do they look like on x-ray?
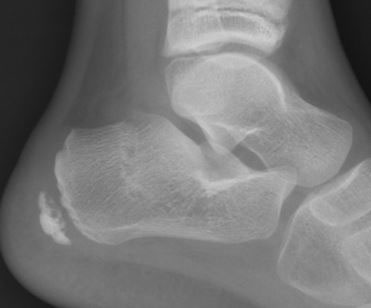
Figure 1: Extra-articular fracture, lateral view
Figure 2: Intra-articular fracture: Depression type. Lateral and Harris views. Note the decrease in Bohler's angle.
Figure 3: Tongue-type intra-articular fracture, lateral and Harris views
Extra-articular tongue-type fracture - this is a surgical emergency due to risk of pressure necrosis:

Figure 4:Tongue-type extra-articular fracture, lateral view
Figure 5: Lateral and axial views demonstrating calcaneus fracture with preservation of Boöhler's angle; the CT reveals t he fracture to be intra-articular (a single sagittal slice is shown here)
Figure 6: Lateral view of fractured calcaneus, appearing to be extra-articular on plain film. A CT reveals the injury to be intra-articular, as shown on this single axial slice.
7. When is reduction (non-operative and operative) required?
Non-operative reduction in the Emergency Department is not indicated.
Displaced intra-articular fractures may require open reduction and internal fixation
Tongue type fractures with tenting of the adjacent skin requires emergent surgery and fixation in order to avoid skin compromise.
Extra-Articular calcaneal fractures, particularly in younger children are often managed non-operatively.
8. Do I need to refer to orthopaedics now?
All calcaneal fractures should be discussed with orthopaedics.
This is particularly urgent for:
- Suspected intra-articular fractures
- Calcaneal avulsion fracture with skin tenting
- Neurovascular compromise
9. What is the usual ED management and follow up for this injury?
|
Assessment for concurrent injuries as part of a complete trauma survey is a core part of ED management.
Vertebral fractures, tibial plateau fractures and additional foot fractures are often associated with calcaneus fractures.
|
- For intra-articular fractures, a well-padded temporary splint in approx 10 degrees plantar-flexion can be applied for whilst arranging orthopaedic consultation as above
- Early CT is sometimes obtained to assess intra-articular displacement, in consultation with orthopaedics.
- Most extra-articular fractures can be managed with immobilisation in below-knee backslab or cast
- most patients will not tolerate dorsiflexion of the ankle and as such, usually won't tolerate a CAM boot acutely. These patients should be splinted in slight (5-15 degrees) plantar flexion initially: a CAM boot can be arranged later through fracture clinic, with a total of 4-6 weeks immobilisation expected.
10. What follow up is required?
Consultation with orthopaedics is advised for cases of calcaneus fracture diagnosed in the ED.
Intra-articular or displaced fractures will have futher management under the orthopaedic unit.
Where all parties agree that the fracture is non-displaced and extra-articular, follow up in the fracture clinic can be arranged in one week with a repeat x-ray.
11. What advice should I give parents?
- Children being discharged with a calcaneal fracture should avoid bearing weight through the affected foot, at least up until the first review in fracture clinic.
- The leg should be elevated whenever possible, particularly during the first week
- Regular simple analgesia (eg paracetamol, ibuprofen) may be required
- The cast/splint should remain on up until review in fracture clinic, with a total of 4-6 weeks immobilisation expected
12. What are the potential complications associated with this injury?
- Skin necrosis and fracture blisters.
- Long term osteoarthritis in intra-articular fractures.
- Delayed diagnosis when occurring with other major injuries in severe trauma.
13. References
Boyle, M. J., Walker, C. G., & Crawford, H. A. (2011). The paediatric Bohler's angle and crucial angle of Gissane: a case series. Journal of orthopaedic surgery and research, 6, 2.
https://doi.org/10.1186/1749-799X-6-2
Inokuchi et al, Calcaneal Fractures in Children, J Pediatr Orthop, 1998; 18(4):469-474
Petit, C et al, Operative Treatment of Intraarticular Calcaneal Fractures in the Pediatric Population, J Pediatr Orthop, 2007;27(8):856-862