NB Text in italics relates to CPR in the context of COVID-19. This applies to any child in whom COVID-19 is
suspected or confirmed . Resuscitation of all other children should be as per usual protocols. Individual State policies should be followed.
See also
APLS algorithms
APLS statement on paediatric resuscitation during COVID-19 pandemic
COVID-19
COVID-19
Emergency airway management
Resuscitation: Hospital Management of Cardiopulmonary
Arrest
Resuscitation: Care of the seriously unwell child
Recognition of the
seriously unwell neonate and young infant
Key points
- Cardiac arrest should be suspected in an infant or child who is unresponsive and not breathing normally - pulse check should not delay cardiopulmonary resuscitation (CPR)
- CPR should be commenced if cardiac arrest is suspected
- Ongoing management should be directed by the cardiac rhythm identified
- Effective resuscitation relies on a coordinated team and good communication
- Children appear to be less likely to transmit COVID-19 to healthcare workers than adults
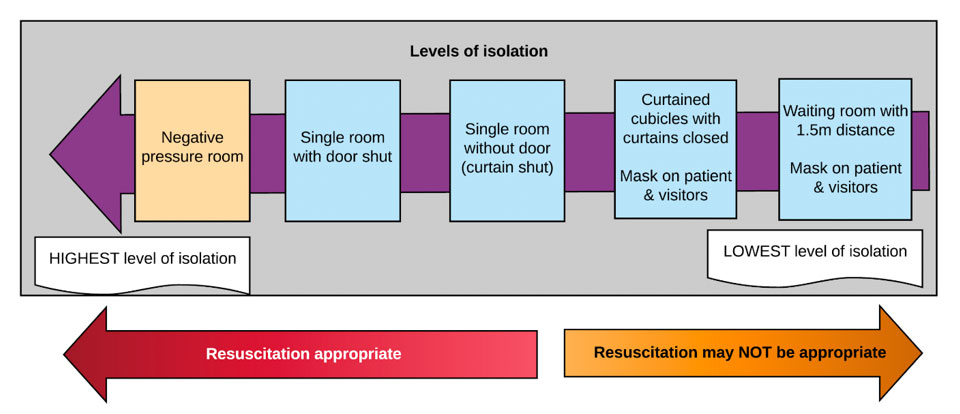
- CPR may cause aerosolisation of virus; airborne precautions (see below) must be initiated as soon as possible and management must occur in the highest level of isolation available (see Levels of isolation diagram below)
- Ideally, CPR should not be delayed for donning of airborne precautions PPE; decisions on providing airway support in the absence of PPE need to be made with the understanding that there may be a small risk of COVID-19 exposure
- If arrest is anticipated, PPE should be donned in advance. If arrest is unanticipated, initial resuscitation, including airway opening, bag valve mask (BVM) ventilation and chest compressions, may be provided by a first responder wearing a mask, gloves and eye protection (at minimum), who should hand over to a staff member in airborne precautions PPE as soon as possible
- Staff at increased risk from COVID-19 should consider not working in the resuscitation room
Background
- The majority of arrests in children are due to hypoxia, hypotension and acidosis
- Children are more likely to arrest from usual causes than COVID-19
- Children appear to be less commonly and less severely affected by COVID-19 than adults
- The most common dysrhythmias are severe bradycardia and asystole
- Ventricular fibrillation (VF) is the initial arrest rhythm in approximately 10%
- Traumatic cardiac arrest is a unique situation - the management is different to non-traumatic cardiac arrest and is not covered by this CPG
- Children need early attention to airway and breathing. To avoid delays in providing resuscitation, initial CPR may be provided by a staff member wearing a surgical mask. Additional staff should wear airborne precautions PPE and take over as soon as possible to continued advanced resuscitation
- Aerosolising procedures that should be managed with airborne precautions as soon as possible include:
- Bag valve mask and anaesthetic t-piece: risk decreased by using a viral filter
- Suctioning using an open system including Yankauer suction tube
- Intubation
- Laryngeal mask airway (LMA) insertion
- Cardiac compressions
- Early allocation of roles can optimise resuscitation (if personnel available); in the setting of COVID-19, personnel should be kept to a minimum and physical distancing should be maintained if possible; restrict personnel to those with most expertise
- Team leader (maintain physical distance if possible)
- Airway nurse and doctor
- Circulation nurse and doctor
- Cardiac compression personnel
- Defibrillator operator (outside the room, with the door shut, unless required)
- Assessment doctor (maintain physical distance when not performing assessment)
- Scribe + time keeper with stop watch (maintain physical distance if possible)
PPE for CPR
Aim for airborne precautions PPE for all responders ASAP
|
|
Minimum precautions |
Airborne precautions |
|
|
Surgical mask, eye protection and gloves |
N95 mask + eye protection + gown + gloves |
|
First responder |
+ |
|
|
Apply oxygen and open airway |
+ |
|
|
Defibrillation (without airway support) |
+ |
|
|
Bag mask ventilation |
+ (initial) |
+ (ongoing) |
|
Suction |
|
+ |
|
Cardiac compressions |
+ (initial) |
+ (ongoing) |
|
LMA insertion |
|
+ |
|
Intubation |
|
+ (incl face shield) |
|
Care of intubated post-arrest patient |
|
+ |
If there is any breach in PPE during resuscitation, affected staff should leave the room and carefully doff and don PPE once again
Resuscitation
Assess for signs of life or response; if they are absent, commence CPR
First Responder may commence airway management without airborne precautions PPE, but should hand over to a staff member in PPE as soon as possible
A – Airway
Look, listen, feel for patency / added noises Avoid close contact with mouth/nose as much as possible
Optimise head position
Consider simple airway manoeuvres (head-tilt chin-lift or jaw thrust)
Suction secretions / blood / vomit ONLY if responder wearing airborne precautions PPE
B - Breathing
Look for chest rise and fall and auscultate
Apply oxygen via face mask at 10 L/min
Commence artificial ventilation with self-inflating bag valve mask or anaesthetic t-piece using 100% oxygen (Add viral filter – see below)
Consider oro / nasopharyngeal airway for upper airway obstruction
Consider 2-person technique for poor mask seal; 2-person technique is preferred
Intubation should be considered for persistent obstructed airway or at some stage during CPR (see
Emergency airway management in COVID-19 context) (see Emergency intubation checklist COVID)
Intubation should be considered early as this may decrease the ongoing risk of aerosolisation
Bag valve mask (BVM) ventilation
- Select appropriate sized resuscitator bag and add viral filter between mask and bag
- Infant up to 2 years - 500 mL bag
- Child/adult >2 years - 2 L bag
- Select an appropriate sized mask
- Obtain airtight seal - use 2-person technique
- Use Oropharyngeal airway to facilitate airway opening and BVM ventilation
- Briefly suction mouth and pharynx ONLY if needed, using a Yankauer suction tube under direct vision
Intubation
- Intubation using a cuffed ETT is preferable to LMA, which is preferable to BVM ventilation
- Insert LMA if expertise in intubation unavailable
- Use CMAC videolaryngoscope if available to move the operator further away from the child’s airway
- Inflate cuff and attach viral filter prior to ventilation
- Minimise disconnection of circuit, and clamp ETT if disconnection is required
- If ongoing suction is required, use in-line suction
- Pass a NG (OG if facial trauma) to decompress the stomach
*If available, continuous wave-form end-tidal CO2 monitoring, should be used to:
- Warn of accidental extubation during CPR
- Monitor for return of spontaneous circulation
- Ensure adequacy of ventilation
C - Circulation
If no signs of life continue CPR
If signs of life assess pulse
Palpate central pulse (brachial, femoral, carotid)
Assessment of pulse can be difficult and inaccurate
If no pulse, slow pulse (<60 in an infant) or unsure, continue CPR
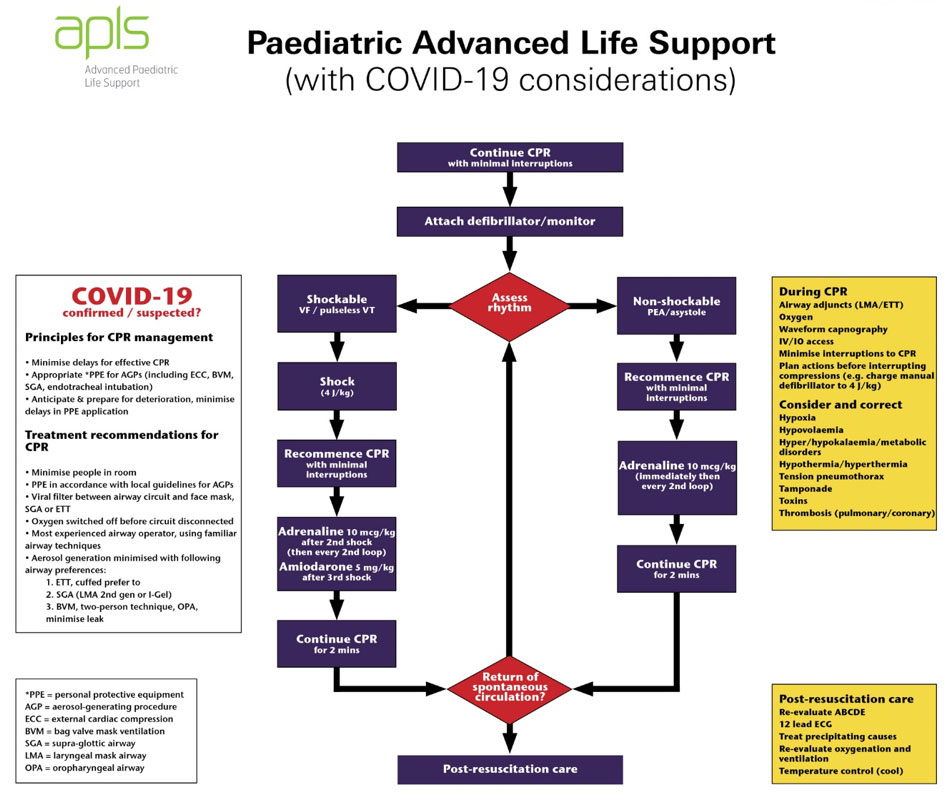
Determine the cardiac rhythm: shockable or non-shockable
(see Advanced Life Support flow chart above)
Technique
External cardiac compression
- CPR rate for all ages 100-120 bpm
- Ratio for CPR is 2 breaths: 15 compressions
- Once intubated, breaths can be at a more normal rate aiming for normocapnia:
- 25 bpm for infants
- 20 bpm for 1-8 years
- 15 bpm for 8-12 years
- 10-20 bpm for >12 years
- Place the child on a firm surface. If on a bed, place the cardiac compression board under the patient, not under the mattress
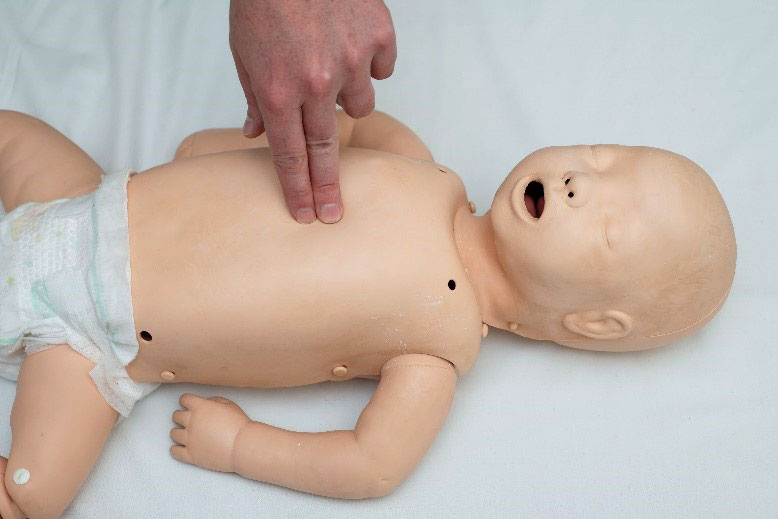
- Perform external cardiac compressions to the lower half of the sternum in all patients including new-borns
- Compress sternum 1/3 the depth of the chest
- Use the hand technique that allows you to achieve this:
For newborn infants the best technique is a two-handed hold in which both thumbs compress the sternum

For infants two fingers may be used
For small children use the heel of one hand

For larger children use the "heel" of one hand with the other superimposed

DO NOT interrupt CPR except for rhythm check or defibrillation
Defibrillator operator instructions:
"HANDS OFF” – pad placement or DC shock – “Continue CPR" – “HANDS ON”
For rhythm check consider “COACHED”
Continue CPR
Oxygen away
All clear
Charge
Hands off
Evaluate rhythm
Defibrillate or ‘dump charge’
- Frequent changes of cardiac compression personnel (every few minutes) is desirable
- Continue CPR until the next designated rhythm check
- Gain IV access as soon as possible
- Consider
intraosseous access early
- If DC shock delivered, recommence CPR immediately for 2 minutes prior to rhythm check
During resuscitation
Correct treatable causes
- Hypoxaemia
- Hypovolaemia
- Hypo/hyperthermia
- Hypo/hyperkalaemia
- Tamponade
- Tension pneumothorax
- Toxins/poisons/drugs
- Thrombosis
Other considerations during resuscitation
- Aim for normal glucose
- Aim for normal carbon dioxide (CO2)
- Aim for normal temperature
- Toxin induced cardiac arrest requires urgent consultation with National Poisons Centre 13 11 26
- Resuscitation for toxin induced cardiac arrest and cardiac arrest following cold-water drowning may be prolonged
Medications for paediatric arrest
Emergency Drug and Fluid Calculator
Monash Book drug doses
|
Drug |
Dose |
Indication |
|
Adrenaline 1:10,000 |
10 microgram/kg =
0.1 mL/kg IV/IM/IO |
Shockable and non-shockable cardiac arrest path
Non vagus-induced bradycardia |
|
Amiodarone |
5 mg/kg IV/IO |
Shock resistant ventricular fibrillation or pulseless ventricular tachycardia |
Atropine, lidocaine, sodium bicarbonate and calcium are only considered in specific situations
Extracorporeal Cardiopulmonary Resuscitation (ECPR)
ECPR is a procedure offered by specialised paediatric intensive care centres in Australia - eligibility should be discussed urgently with local retrieval service
Post resuscitation care - following return of spontaneous circulation
- Re-evaluate ABCD
- Ensure airway and breathing are managed effectively, including intubation if not already performed; do not extubate
- Titrate inspired to achieve normal saturations, avoid excessive oxygenation
- Ventilate to normal CO2
- Perform CXR to confirm ETT in desired position and check for complications of CPR (pneumothorax, rib fractures, aspiration)
- Maintain normal blood pressure appropriate for age with use of inotropes as needed
- Perform 12 lead ECG
- Monitor for further arrhythmias and consider ongoing anti-arrhythmic medication
- Consider echocardiography to monitor contractility and exclude tamponade
- Check haemoglobin, pH, electrolytes and glucose and correct as necessary
- Aim for normal temperature (avoid hypo/hyperthermia)
- Use adequate sedation and analgesia
- Test for coronavirus once patient is stable: PCR of throat and nasopharyngeal swab using same swab, and of the lower respiratory tract
Withdrawal of CPR
The decision to withdraw CPR in children is difficult and must involve senior experienced clinicians who will consider the clinical context and the desires of patient and family
Family and staff support
Family members of patients undergoing resuscitation should be given the option to be present, ideally with an assigned support person. Most hospitals are likely to have a family presence policy and staff education strategy in place, which is likely to have been adapted for COVID-19. Family members may be asked to observe from outside the room, and the assigned support person should most likely be a staff member. PPE may be required
Regardless of the outcome, resuscitation is stressful and can be psychologically traumatic to team members providing care. Debriefing and support should be offered to all involved staff who wish to attend
For emergency advice and paediatric or neonatal ICU transfers, see
Retrieval Services
Additional notes
ID badge size Resuscitation Card
New Zealand Resuscitation Council Paediatric ALS Support for COVID-19 patients
Respiratory Support for children during the COVID pandemic (SCV)
Neonatal resuscitation in suspected or confirmed cases of COVID-19
Resuscitation Council UK Paediatric advanced life support algorithm
Last updated January 2022