Factors affecting remodelling
Due to the presence of growth plates, the healing of fractures in children is often much faster than in adults and is followed by a process of fracture remodelling.
Factors affecting the remodelling capacity include:
Age
The rate of remodelling in a child is inversely related to age (Figure 5). In younger children, remodelling is rapid and often complete. It is slower in older children and much slower in adolescents.
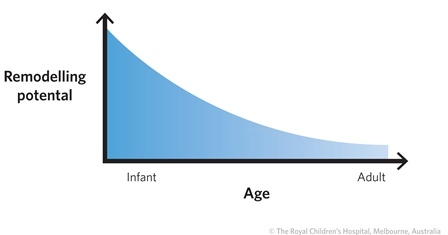 |
| Figure 5: The rate of remodelling is inversely related to age. |
A key is the number of years of growth remaining, from the time of injury to physeal closure. On average, physeal closure occurs in boys at age 16 and in girls at age 14 but there is a wide variation around these means. It is sometimes wise to formally check the bone age from a radiograph of the wrist or elbow than to rely on chronological age (Figure 6).
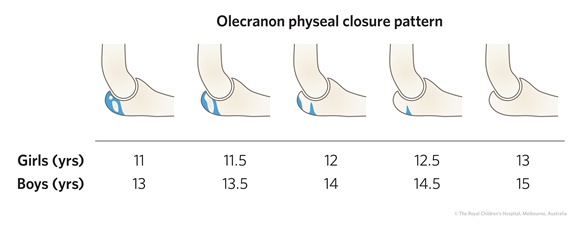 |
| Figure 6: Olecranon physeal closure pattern. |
Fracture site
Fractures close to the ends of long bones remodel much faster than those in the mid shaft. Therefore physeal injuries remodel faster than metaphyseal injuries, which in turn remodel faster than diaphyseal injuries. But there is also an influence on which end of the long bone is injured. The different rates of remodelling follow the rate of growth at the ends of the bone. In the upper limb, the most active growth plates contributing to longitudinal growth are those of the proximal humerus and distal radius and ulna (Figure 7). Hence, injuries of the proximal humerus and fractures close to the wrist remodel much faster than injuries of the elbow and proximal forearm. The reverse is true in the lower limb. Remodelling is fastest at the knee (distal femur and proximal tibia) than in the proximal femur and distal tibia (Figure 7).
Figure 7: Skeletal homunculus depicting the relative contributions of the growth plates to the longitundinal growth of the upper and lower limb.
Relationship to joints
Remodelling is maximal in proximity to, and in the plane of action of, the nearest joint. The shoulder is a ball and socket joint; it moves in three planes and remodels in three planes. At least 30 degrees of angulation (in any direction) is acceptable in a child with more than two years of growth remaining. This is in contrast with fractures near the elbow, which is a hinge joint. Sagittal plane displacement remodels slightly but very slowly. Coronal plane displacement does not remodel at all. The cubitus varus or "gunstock" deformity after supracondylar fracture must be prevented because it will not remodel (Figure 8).
Figure 8: Cubitus varus (red arrow) deformity of the elbow can result from malunion of a supracondylar humeral fracture. The normal carrying angle of the arm is reversed and the forearm deviates to the midline when the elbow is extended. It does not result in much functional limitation but it is a serious cosmetic problem which can lead to litigation.